Innovations | Vaginal Prolapse Buckinghamshire
Total Laparoscopic Hysterectomy
Prolapse Repair with Mesh
Intravesical Botox Treatment
Sacrospinous ligament fixation
Laparoscopic Sacrocolpopexy
Tension Free Vaginal Tape (TVT)
Laparoscopic uterine suspension (laparoscopic sacrohysteropexy)
Prolapse Surgery
Surgical options for patients with uterine and/or vaginal prolapse is dependent upon:
-
Degree or severity of prolapse
-
Areas specific for prolapse
-
Desire to maintain fertility (maintain uterus)
-
Desire to maintain sexual function
-
Patients age
-
Patients overall general health
-
Patients desire and opinion
Mr Fayyad has been trained to perform the prolapse repair procedures through multiple approaches such as:
Vaginally (through vagina)
Laparoscopically (mini-incisions) and Laparotomy (Large abdominal incision)
Mr Fayyad chooses to perform these procedures through the least invasive way possible for each individual patient.
In an attempt to restore vaginal anatomy, maintain sexual function and address urinary leakage, difficulty emptying bladder, and defecatory function, sometimes more than one surgical procedure are performed on the patient during one operation. This is done in an attempt at minimizing vaginal and uterine prolapse recurrence and therefore subsequent surgery.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair.
Laparoscopic Hysterectomy
As an advanced laparoscopic surgeon, Mr Fayyad performs total laparoscopic hysterectomy and laparoscopically assisted vaginal hysterectomy in women with heavy periods, painful periods and endometriosis. These procedures are now performed through 3 small abdominal incisions and the whole uterus is removed via key-hole surgery. The advantages for patients are immense, including one night hospital stay, quicker recovery and return to normal activiities including early return to work. In the days of modern surgery, this procedure should be the standard procedure for women who need hysterectomy for period abnormalities.
For further information about recovery following laparoscopic hysterectomy, please visit www.rcog.org.uk/ recovering-well, and click on laparoscopic hysterectomy.
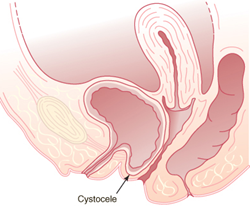
Anterior Repair
This procedure is performed in women suffering from prolapse of the front wall of the vagina (Figure 1). The procedure is performed under general anaesthetic, or spinal (epidural) anaesthetic. Occasionally it can be performed under local anaesthetic. The procedure involves putting your legs in stirrups, infiltration of the vaginal skin with local anaesthetic, followed by incision of the vaginal skin and the thin layer of muscle in the vagina. After that, the layer of muscle is brought together with a series of strong sutures and the vaginal skin is closed.
You will have a vaginal pack and catheter over night. The catheter will come out the next morning and you should be able to go home once you resumed normal voiding. The operation is generally safe, but occasionally women develop infection or bleeding after the operation. Also women may develop some difficulty passing urine initially. This tends to settle down with time. In 5-10% of the cases, the prolapse may come back needing further treatments. You may notice sutures coming out of the vagina in few weeks time. This is normal as your body is healing.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair.

Vaginal Hysterectomy
This procedure is performed in women with prolapse of the womb, to achieve good elevation of the top of the vagina. The procedure is done under general anaesthetic or spinal (epidural anaesthetic). It involves a cut in the vagina (not in the abdomen) followed by removal of the womb. The vaginal skin is closed afterwards and a pack and catheter inserted over night. They should come out in the next morning and you can expect to go home next day or the day after. We normally perform a repair operation at the same time of the hysterectomy. If you wish to avoid a hysterectomy, we have the unique expertise of providing key-hole prolapse surgery with preserving the uterus. See under laparoscopic uterine suspension (sacrohysteropexy).
For further information about recovery following this operation, please visit www.rcog.org.uk/ recovering-well, and click on vaginal hysterectomy.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair.
Posterior Repair
This procedure is performed in women suffering from prolapse of the back wall of the vagina (Figure 2). The procedure is performed under general anaesthetic, or spinal (epidural) anaesthetic. Occasionally it can be performed under local anaesthetic. The procedure involves putting your legs in stirrups, infiltration of the vaginal skin with local anaesthetic, followed by incision of the vaginal skin and the thin layer of muscle in the vagina over the prolapse. After that, the layer of muscle is brought together with a series of strong sutures and the vaginal skin is closed.
You will have a vaginal pack and catheter over night. The catheter will come out the next morning and you should be able to go home once you resumed normal voiding. The operation is generally safe, but occasionally women develop infection or bleeding after the operation. In 5-10% of the cases, the prolapse may come back needing further treatments. You may notice sutures coming out of the vagina in few weeks time. This is normal as your body is healing.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair.
Perineoplasty
This is an operation to tighten and rebuild the introitus (entrance to the vagina). Many women feel that the entrance to the vagina is loose which is mostly precipitated by childbirth. The operation involves approximating the muscles near the entrance to the vagina along with repair of the skin over it with sutures. You may experience pain following surgery, but this tends to settle down with time.
Mesh Vaginal Repairs
Mr Fayyad is one of few urogynaecologists in the UK performing mesh vaginal repairs for women with prolapse. Generally, the current indication is in women with recurrent prolapse (i.e. had previous prolapse treatment that did not work). Mr Fayyad uses the ELEVATE PC vaginal mesh kit in this select group of patients. Mr Fayyad has published his own experience in the use of this mesh system which is the longest follow up study currently published.
Mesh repair is generally safe and up to 89% of women feel much better following surgery as the prolapse is cured. Patients, however, may experience mesh exposure in the vagina, which is rare (1-5%) and easily treated. Majority of women, however, feel that their sexual function improves following this procedure due to disappearance of the prolapse.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair.
Intravesical Botox Treatment
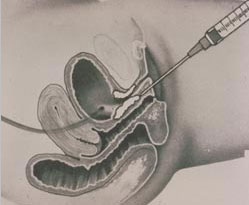
This treatment is reserved for women with overactive bladder (OAB), with symptoms of urgency, frequency and urgency incontinence who failed to respond to conservative treatment, that includes fluid management, bladder retraining and medications. The procedure is quick and done as a day-case procedure. Patients can have either general anaesthetic, epidural anaesthetic, or local anaesthetic. A very fine needle is inserted into the bladder with the telescope (cystoscope), and Botox treatment is injected into 15-20 sites in the bladder wall. This treatment is very successful in treating women with overactive bladder symptoms with expected significant improvement in 80-90% of women. The treatment can result in slight problem in emptying the bladder in 10-20% of women that tends to resolve over time. Patients generally will need repeat treatments every 9-12 months to stop the symptoms coming back. Mr Fayyad is fully trained to provide this treatment for women with OAB, with excellent success rate, and day-stay procedure.
Cystoscopy
The operation can be done under general anaesthetic, spinal anaesthetic or local anaesthetic gel instilled into the urethra (the water pipe). You may have a choice of which anaesthetic is used. A spinal anaesthetic involves an injection low in the back, similar to what we use when women are in labour or for a caesarean section. The spinal anaesthetic numbs you from the waist down. This removes any sharp sensation but a pressure sensation may still be felt. Local anaesthetic gel instillation into the urethra. This may take few minutes to work and is generally installed 5 minutes or so prior to the cystoscopy. The legs are placed in stirrups (supported in the air).
The lighted telescope (cystoscope) is introduced gently into the urine pipe and the bladder. A camera may be attached to the end of the cystoscope and the inside of the bladder is examined accordingly (Figure 1). Occasionally, a biopsy (small tissue sample) of the bladder wall is taken to be examined in the laboratory. This is done through a fine grasping instrument introduced through the cystoscope. Occasionally, electrical energy is needed to stop the bleeding if it develops from the bladder wall as a result. This is called diathetrmy.
There are two types of cystoscopes; the rigid cystoscope which is made of metal (Figure 1), or the flexible cystoscope, which is finer and could be used while the patient is awake (Figure 2)
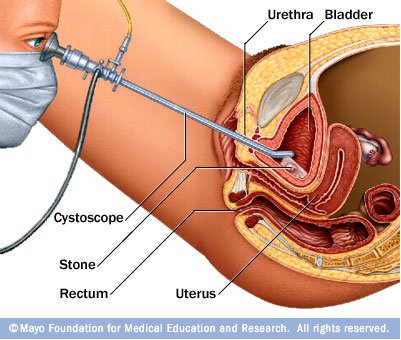
Figure 1. Cystoscopy
-
In more than 95% of cases, the operation is done as a day case, meaning you can go home on the same day.
-
On return from the operating theatre you may have a fine tube (drip) in one of your arm veins with fluid running through to prevent you becoming dehydrated.
-
You may have a tube or catheter draining the bladder overnight if a bladder biopsy was taken (see above). The catheter may make you feel as though you need to pass urine.
-
The nurses will advise about sick notes, certificates etc.
-
The doctors or nurses will discus with you the findings of the operation and advise you on follow up.
-
When you arrive home you must continue to potter around.
-
You are likely to feel tired and may need to rest in the daytime from time to time for a week or so. You will gradually improve.
-
You can drive as soon as you can make an emergency stop without discomfort.
-
You can start sexual relations whenever you feel comfortable enough.
-
Follow up after the operation may be from six weeks to six months and dependant on the circumstances will be at the hospital with the doctor or a specialist nurse or by your GP or phone.
-
Drink plenty of water / juice
Urinary Incontinence
Tension-Free Vaginal Tape (TVT sling) Sling
The goal of surgery for stress urinary incontinence is to stop urinary leakage and this is accomplished by supporting the urethra. The urethra is the tube that allows urine to be expelled from the body. In an attempt to support the urethra, the vagina under and beside the urethra is the area which the operation takes place. This procedure is commonly called the SLING.
Mr Fayyad have been trained to perform a number of different types of sling operations utilizing various types of material, sutures and points of anchoring. Currently he chooses to offer their patients an extremely minimally invasive sling operation known as the TVT sling or tension free vaginal tape sling.
This TVT procedure has been performed in Europe for more than 12 years with great success. Mr Fayyad serves as a preceptor to teach this operation to Urologists, Urogynecologists and Gynecologists throughout the world. In August 2009, Mr Fayyad travelled to Jordan to introduce the TVT sling operation to his colleagues at the University of Jordan.
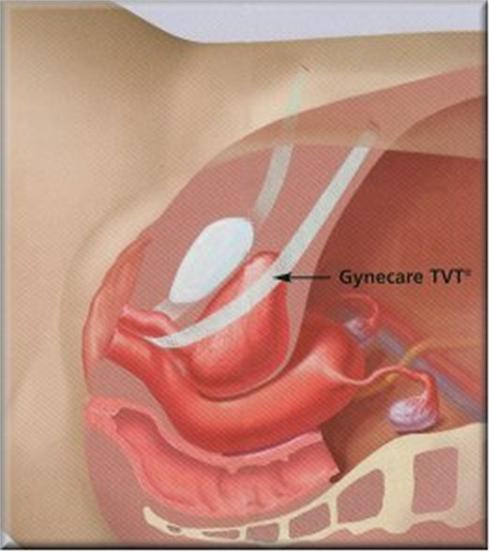

Figure 2: TVT sling
The operation has the following advantages:
-
Minimally invasive (two incisions of 1/3 inch on the pubic hairline)
-
Minimal pain (40% of patients will not need a pain reliever after 24 hours)
-
Proven cure rate of 86%
-
Same day or next day discharge for 98% of patients
-
Performed under local anesthesia and IV sedation
-
Operative time 20-30 minutes
-
Minimal postoperative need for catheterization
-
Minimal complications which include voiding dysfunction, mesh erosion and urinary urgency
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on mid urethral sling procedures.
Bulkamed Injections
Collagen is a naturally occurring protein found in humans and animals and supports the closure mechanism of the bladder. When Bulkamed is injected into the tissue around the urethra, it adds bulk and helps it close tightly to prevent urine leakage, especially urine leakage associated with activity (Stress Urinary Incontinence). Most patients will leak much less or not leak at all after collagen therapy. Some patients will need to have one or more injections done at a later date because the body will absorb some of the collagen material. The length of time between injections varies with each patient. Some need to be re-injected after a few months and some after a few years.
The procedure could be done under local, spinal (like epidural injection) or general anaesthetic. It is mostly suitable for elderly women who are not fit for more invasive treatments or women who had previous failed incontinence surgery.
Incontinence Treatment: Figure 2
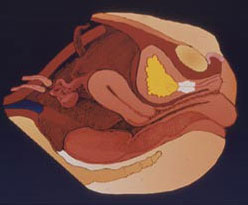
Incontinence Treatment: Figure 3
Bulkamed Injection - Used for bulking up and tightening the urethra. This is a minimally invasive technique of treating stress urinary incontinence.
Laparoscopic Uterine Suspension (Laparoscopic sacrohysteropexy)
Traditional medicine recommends removal of the uterus (hysterectomy) when there is uterine prolapse. In cases of severe uterine and vaginal prolapse a hysterectomy followed by vaginal wall reconstruction may still be the most beneficial therapy. However there are more women who are electing to keep their uterus especially in those whom the uterus is only mildly or moderately prolapsed. The decision to attempt uterine and vaginal support is made only after a full informed consent is made with the patient having the operation. One of the most important aspects of this surgery is the lack of long term data supporting its utilization in uterine and vaginal prolapse surgery.
There are many methods of uterine suspension including sacrospinous tailbone) and uterosacral ligament suspension. Mr Fayyad routinely performs the laparoscopic approach and/or utilizing mesh to suspend the uterus (sacrohysteropexy Figures 1 and 2) or in some cases the uterosacral ligaments.
In the laparoscopic sacrohysteropexy with mesh, The cervix is grasped by special forceps. An incision is then made in the vaginal skin surrounding the cervix and a soft nylon mesh is then sutured to the cervix (Figure 4) and the vaginal skin closed over it (figure 5). The mesh is then secured to the sacrum (tailbone) through key-hole surgery (Figure 6) after reducing the prolapsed uterus. Then mesh is then buried using laparoscopic suturing techniques (Figure 8).
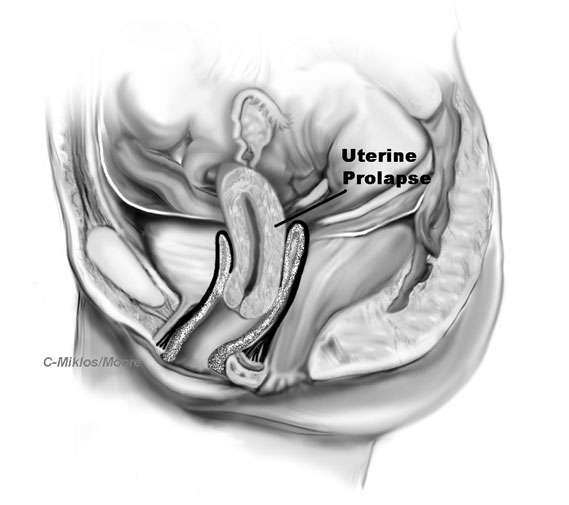
Figure 1: Diagrammatic presentation of uterine prolapse
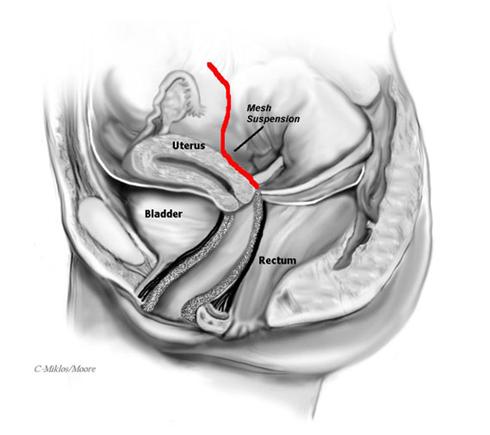
Figure 2: Sacrohysteropexy with mesh attaching the cervix to the sacrum
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair, and laparoscopy.
Laparoscopic sacrocolpopexy
The abdominal sacral colpopexy is one of the most successful operations for vaginal vault prolapse with excellent results. It involves suturing a synthetic mesh that connects and supports the vagina to the sacrum (tailbone). This procedure is complex in its nature and requires great expertise for a favorable outcome. Mr Fayyad has been performing the laparoscopic sacral colpopexy in the same manner as an open procedure with the exception of using a laparoscope over the past 5 years.
Advantages
By performing the sacral colpopexy laparoscopically, the vagina is repositioned to its anatomic position in a minimally invasive manner. Most surgeons perform this procedure through a large incision thus contributing to a longer recovery time. Our laparoscopic approach also allows us to incorporate additional laparoscopic procedures if needed.
Mr Fayyad can perform the laparoscopic sacral colpopexy in less time, less blood loss, smaller incisions and perform the surgery more precisely than by doing it through an open laparotomy. There are only very few centres in the country offering this procedure through the laparoscopic approach.
Surgical Technique for Laparoscopic Sacral Colpopexy
After placing two to three small incisions in the abdomen, the acces ports are placed, the bowel is mobilized out of the deep pelvis and the sacrum (tailbone) is identified. The peritoneum over the sacrum (tailbone) is elevated and then incised.
A vaginal probe is placed into the vagina to elevate the apex or vaginal vault into the surgical field.
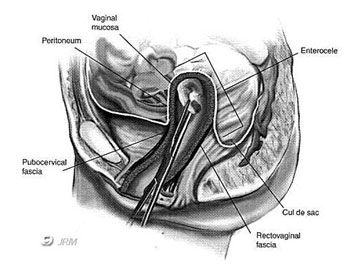
Figure 1 -- Vaginal vault (apex) : Probe holds vagina up from below
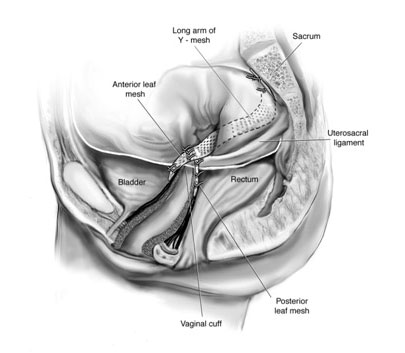
Figure 6- lateral view of mesh attached to the both anterior wall and posterior wall of vagina and then to the sacrum (tailbone)
The peritoneum covering the apex of the vagina is incised and the bladder is dissected away from the top of the vagina anteriorly and the rectum dissected away posteriorly.
A piece of mesh which is shaped like a Y (Figure 5) is then attached both to the posterior aspect of the vagina, the vaginal apex and the anterior vaginal wall which normally supports the bladder. The mesh is then secured to the sacrum (tail bone) by strong staples (Figure 6).
Results/Complications
This procedure has excellent success rate with low complication rate.
Some of the complications that can occur during Sacral Colpopexy include:
-
Mesh Infection
-
Mesh Erosion
-
Bleeding
-
Pain with intercourse
The most common risk of the use of mesh at the top of the vagina, is mesh extrusion through the vaginal skin, which is typically a minor complication, but one that does need a procedure to excise the exposed mesh and repair the skin where it came through. This risk exists whether the procedure is completed through an open incision or the laparoscope.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well, and click on pelvic floor repair and laparoscopy.
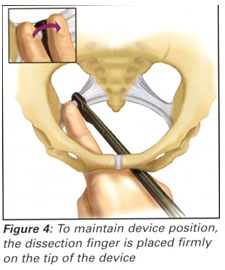
Sacrospinous Ligament Suspension
The sacrospinous ligament suspension fixation (SSLF) procedure is a less invasive and moderately successful operation for vaginal vault prolapse. This procedure is suitable for some patients that would not be candidates for laparoscopic or abdominal surgery or were felt to be better candidates for a vaginal approach under epidural anesthesia
The sacrospinous ligament technique is described below. Images are from Technique Spotlight Suture Placement, Vol. 3, by Boston Scientific featuring the use of the Capio (TM) Suture Capturing Device. The procedure is completed vaginally.
Sacrospinous Ligament Fixation Suture Placement
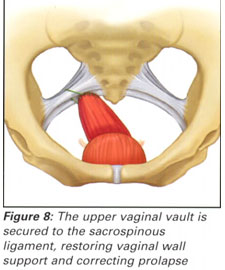
Vaginal Support with Sacrospinous Ligament Fixation
Results/Complications
This procedure should only be completed by experienced advanced pelvic surgeons. Risks include bleeding or hematoma in the pararectal or retropubic space (depending on posterior or anterior approach), injury or irritation to the pudendal nerve (buttock or leg pain).
As stated previously, many surgeons may not complete a vaginal vault suspension at the time of prolapse surgery, even if the patient has vault prolapse, because of the difficult and complex nature of the procedures reviewed above. This can lead to problems such as a shortened vagina, pelvic pain, painful intercourse, urinary symptoms (urgency, frequency, nocturia, difficulty emptying) that can occur post-operatively if the vaginal vault wasn’t properly suspended.
For further information about recovery following surgery, please visit www.rcog.org.uk/ recovering-well and click on pelvic floor repair.